
Scientific Evidence for AlkaPlex® (formerly Alka-Plex®)
The Patented Creation of the AlkaPlex® Granule, and Its Benefits
The AlkaPlex Granule
AlkaPlex has two distinguishing characteristics:
- It reduces acidity in foods and beverages without damaging flavor; and
- When ingested it works to balance the complex and critical acid-alkaline relationship in the human body
The Structure of the Granule
AlkaPlex granules are made by using microscopic calcium carbonate carrier particles to hold extremely reactive magnesium hydroxide, potassium chloride and potassium hydroxide (i.e. magnesium and potassium salts). Calcium carbonate is chosen because it does not react with the magnesium and potassium salts and is a stable carrier for those components. The microscopic carrier particles are coated with micro-crystalline cellulose and croscarmellose sodium. Then the particles are assembled into granules. Diagram 1 is a schematic AlkaPlex granule.
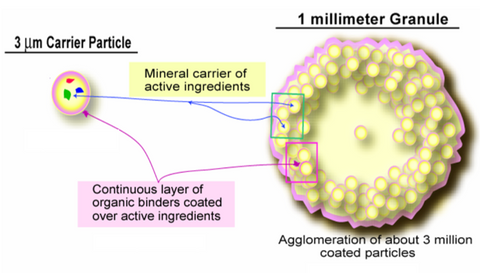
The particular characteristics of the AlkaPlex granule are built upon a central paradigm of material science that the structure (not the composition) largely controls the functions of the material. This is a concept that the discipline of chemistry often finds difficult to evaluate.
The above schematic representation of the AlkaPlex granule shows the microscopic calcium carbonate carrier particle; impregnated with unaltered, stabilized magnesium and potassium salts; coated with micro-crystalline cellulose and croscarmellose sodium; and then assembled into a granule.
Granule Characteristics
The AlkaPlex granule is unusually resilient. It does not disintegrate into a powder when pressed. The highly reactive salts are held in a matrix and are slow to react. As a result, the product has an extraordinarily long shelf life (well in excess of the FDA mandatory three-year maximum). The slow reactivity of the crystal is an important element of the product’s effectiveness. A comparison of the AlkaPlex titration curve and the sodium bicarbonate (NaHCO3) titration curve is a good indication of this (see the two diagrams immediately below).
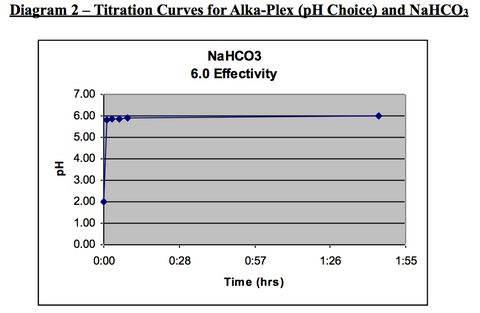
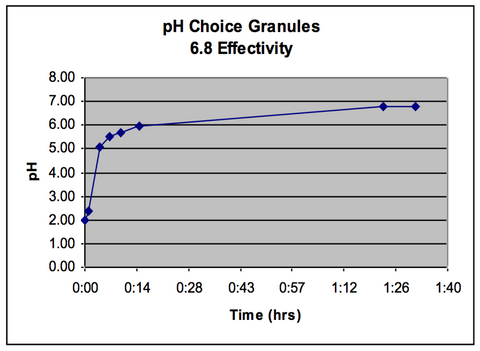
The test starts with two beakers each with 150ml of room temperature hydrochloric acid (HCl) with standard 2.0 pH. Exactly .37 grams of AlkaPlex is added to one beaker and the same amount of sodium bicarbonate is added to the second beaker. The alkaline materials raise the pH levels of the hydrochloric acid over a period of time. The change in acidity is called the titration curve. The resulting titration curves reveal interesting contrasts between the materials:
- AlkaPlex granules release the alkalizing agents in two gradual steps whereas the bicarbonate is one, almost instantaneous, reaction.
- AlkaPlex granules are tasteless and quickly neutralize the acids in foods and beverages. Bicarbonate is very difficult to blend with any food.
- Bicarbonate produces gas while neutralizing hydrochloric acid which, if released in the gut, produces discomfort. AlkaPlex seldom produces gaseous discomfort.
- The first gradual AlkaPlex release takes about 15 minutes to raise the pH of hydrochloric acid to 6.0. This is about the same acid neutralizing power as sodium bicarbonate. But, sodium bicarbonate raises the pH of hydrochloric acid in seconds, not minutes.
- The second AlkaPlex release takes about one hour to raise the pH of hydrochloric acid to 6.8 (7.0 is neutral). Bicarbonate has no such second release.
- For comparison purposes, AlkaPlex removes about seven times (7x) more free H+ ions than bicarbonate.
- The gradual release of the AlkaPlex alkalizing agents probably results in greater absorption of alkalizing agents in the blood and through the intestinal tract. Therefore, significantly less AlkaPlex is needed to impact body pH than is the case with bicarbonate.
- The hydroxyl ions (OH-) in AlkaPlex are likely to be transported and absorbed through the small intestine more readily than the bicarbonate ion (HCO3-) due to the much smaller ion size and the more gradual release of the AlkaPlex ions.
Coffee is an excellent example to describe the potential demand for AlkaPlex as a food acidity reducing product. It is estimated that 35-40 million American adults have decreased or eliminated coffee consumption because of stomach discomfort. Certain coffee acids damage stomach mucosal membranes. AlkaPlex neutralizes those very reactive acids without damaging flavor-causing compounds in the coffee. AlkaPlex makes the coffee more stomach friendly without damaging flavor.
Similarly, wine, tomato-based products, and certain salad dressings are seeing decreased consumption among baby boomers. The unifying reason is sensitivity to dietary acids.
Dietary changes over the last two centuries have resulted in a mismatch with genetically-determined nutritional requirements in humans. Estimates of the net systemic acid load on contemporary humans, when compared to the diet of pre-agricultural Homo sapiens, leads researchers to conclude that contemporary diets generate diet-induced arterial blood pH that ranges in the lower levels of “normal” and are referred to as “low-grade metabolic acidosis.” As a result, wide-spread, chronic low-grade metabolic acidosis is becoming prevalent in athletes and many persons over 30 years old.
AlkaPlex granules do not dissolve completely. As a result, they can leave water, coffee and other drinks with a slightly cloudy appearance, which does not impact taste whatsover.Broad AlkaPlex Benefit 2 - Improving Performance in Competitive Athletes
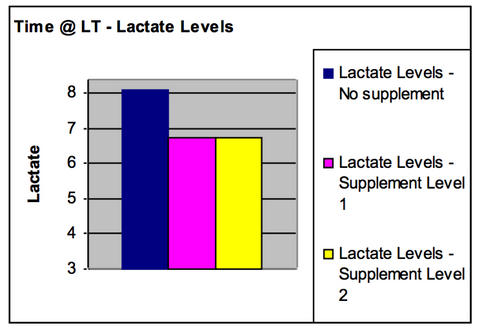
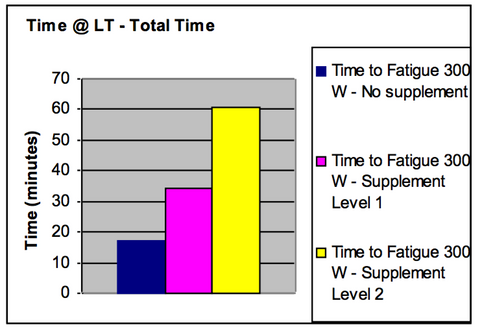
Based on tests given to healthy athletes, AlkaPlex has been shown to help balance the complex mechanisms regulating pH levels and fundamental biochemical functions in the human body. In a pilot study with one competitive athlete, a medical doctor measured blood lactate levels in the athlete working to exhaustion. Blood lactate levels rise as muscle pain and fatigue sets in. Diagram 4, entitled “Lactate Levels of a Competitive Athlete Working to Exhaustion,” shows the lactate levels after an athlete had worked to complete exhaustion on three efforts.
The last two efforts, the athlete was taking AlkaPlex. AlkaPlex has a clear physiological impact on reducing the athlete’s blood lactate levels and hence muscle pain at complete exhaustion. Diagram 5, entitled “Work Performed by Same Competitive Athlete Working to Exhaustion” indicates the athlete performed considerably more work before reaching exhaustion while taking AlkaPlex.
The conclusion is that athletes, soldiers, and others working under severe physical stress may not tire as quickly and may have untapped reserves available to them if they are taking AlkaPlex.
The “wall” that marathon runners hit after 20 miles of running may be moved out considerably. The U.S. Anti-Doping Agency (USADA) has reviewed the AlkaPlex composition and has determined there are no prohibited ingredients in the product. Tests have shown improved endurance and stamina, faster muscle recovery, and less pain and less cramping in athletes taking various doses of AlkaPlex.
What works for healthy athletes also works for an aging population that is beginning to “feel” its age.
Broad AlkaPlex Benefit 3 – Improving Health of an Aging Population
A healthy human body works best, and its chemistry functions most effectively, when it is slightly alkaline. Blood pH in a healthy body lies within a narrow alkaline range of 7.35 to 7.45. “Chronic, low-grade acidosis” arising from excess dietary acids must be distinguished from “acidosis.”
Acidosis is a medical condition which occurs from a pH imbalance where blood pH drops below 7.35. Acidosis is life threatening.
The human body performs heroic measures and compromises essential functions to keep blood pH in the narrow range of 7.35 to 7.45 pH. Therein lays many of the health problems that arise with “chronic, low-grade acidosis” associated with aging.
As we age, body functions become less efficient. Organs and body systems do not work as efficiently as they do for young people. The healthy acid/alkaline balance can easily lean toward too much acid creating acidic stress on the body.
Also, metabolic events—ranging from marathon running to traumatic ailments—can unsettle the acid/alkaline balance. When the body’s pH balancing systems are stressed the body reacts to keep blood pH levels within the low/normal range of 7.35. When this acidic stress is persistent, the condition is described as “chronic, low-grade acidosis.”
Root Cause Response has several AlkaPlex based products that relieve distress in certain body systems caused by chronic, low-grade acidosis. These broad applications arise from a systemic acid imbalance that is present in most people over 30 years old and is increasingly evident among people over 40.
pH Balancing for the Digestive System
We have the first new (patented) antacid in over twenty (20) years based on the AlkaPlex formula. Current antacid formulas are really buffers and rely on large amounts of calcium carbonate. Calcium may make the stomach feel better but it is a mere palliative. Worse, slow-acting but widely advertised proton pump inhibitors are detrimental to the digestive process and contribute to acidic stress.
RCR's "Digestion" formula is an extremely powerful alkalizing agent (eleven times more powerful than extra-strength TUMS® and has essential minerals and considerably less calcium than any other antacid (there is increasing evidence that U.S. consumers are beginning to overdose on calcium). It improves and strengthens the digestive tract while providing immediate relief from acid indigestion.

Lower Digestive Tract Health
AlkaPlex, if delivered in correct doses and dissolve rates, is an effective agent to improve intestinal tract health and reduce the diarrhea and abdominal pain symptoms of certain symptoms associated with irritable bowel syndrome (IBS). IBS effects up to 15% of the population in Western countries and increases frequency with age. Pre-clinical trials are in the planning stage with a major naturopathic university.
Urinary Tract Health
If delivered in correct doses and dissolve rates, AlkaPlex is an effective agent in reducing the symptoms of frequency and urgency of urination. About 68 million people in the U.S. suffer from urgency and frequency symptoms. The initial product tests targeted persons suffering from interstitial cystitis (IC), a particularly troubling condition with urinary urgency and frequency.
There are three primary symptoms of IC—urinary frequency (i.e. a need to urinate as often as every 20 minutes day and night), urinary urgency (i.e. an immediate, compelling need to urinate) and pelvic pain. IC is primarily a condition of middle aged women and often follows a traumatic event or child birth. There is no identified cause of IC and there are no effective cures for the condition. Urinary urgency and frequency is reduced by 34% within two weeks of taking Alka-Plex for most IC sufferers.
The following diagram shows data from a field study of a product, pH Control, made from AlkaPlex, given to persons diagnosed with IC.

Gum Health
When delivered in a test toothpaste form, AlkaPlex is an effective agent in reducing inflammation, infection, and bleeding in gums. Abnormal gum bleeding is often prevalent in persons with chronic, low-grade acidosis and is also associated with aging. Three studies, including a double blind, placebo-controlled study at the University of Washington, has shown that an AlkaPlex based toothpaste reduces gum bleeding in as fast as two weeks. The data from one study is presented below.
In that study, ten subjects with severely bleeding gums (an average of 122 bleeding points) were asked to brush once a day with AlkaPlex toothpaste. Bleeding was reduced to an average of seven (7) bleeding points.

Joint Health
AlkaPlex is added to the diet. This eliminates the need for drugs and their serious negative effects on heart health.
AlkaPlex for Increased Absorption of Nutraceuticals
AlkaPlex, when combined with other botanical dietary supplements can improve the absorption of those products. For example, an important active ingredient in garlic (allicin) is quickly broken down by stomach acids. If it is combined with AlkaPlex, the stomach acids are neutralized, absorption is improved and over thirty (30) times more allicin is absorbed by the body.
pH Balancing for General Health
We are planning on releasing a group of products that promote healthy aging. As humans age, their ability to neutralize acids at the cellular level is reduced. Certain fundamental chemical functions in the body are changed or stop if intra- and inter-cellular pH levels tend toward 7.35. Highly acidic foods compound the problem. Wide-ranging ailments can begin to appear if intra- and inter-cellular acid/alkaline relationships are out of balance. Considerable research is being done in this area. About 4.5 million people turn 50 every year in the U.S. Baby boomers are turning toward health as a major concern. Baby boomers are driving a trend toward healthy aging just as they have driven many U.S. trends in the past.
Maintaining Health
After age 40, a metabolic pH imbalance often begins to appear in a person’s body. That imbalance—chronic, low-grade metabolic acidosis—is associated with chronic discomfort in a wide range of body functions that are associated with the “aging process.” These symptoms do not have to persist because AlkaPlex granules, when delivered appropriately will alleviate many of the most troubling symptoms naturally.
Improving Energy: AlkaPlex, when taken in appropriate doses, increases energy levels and reduces muscle fatigue and soreness that often accompanies physical exertion.
Additional AlkaPlex Research Articles
· Acidosis - An Old Idea Validated by New Research
· Summary of AlkaPlex Scientific Data
· AlkaPlex Research Technical Data
· Exercise and Metabolic Acidosis
· Cooper Sports Elite Bicyclists Final (AlkaPlex) Report
· AlkaPlex Effect on Urine Acid
· AlkaPlex Safety References
Structure-Function Claims for AlkaPlex with Scientific Documentation
| Benefit | Scientific Documentation | |||
|---|---|---|---|---|
| AlkaPlex granules are safe when used as directed. | Food & Drug Administration. 2006. Grant New Dietary Ingredient (NDI) status to AlkaPlex®. Schindler-Horvat, J, Parman, T, Green, C.E. Acute Oral Toxicity of a Nutraceutical (Alka-Plex Granules) in Male and Female Sprague-Dawley Rats. Stanford Research Institute study M384-05, July 2005 Schauss, A. MEM Endpoint Dilution Using L-929 Mouse Fibroblast Cells assay. American Institute for BioSocial and Medical Research (AIMBR) and AppTec Laboratory Services, May 2004 Brown, S. Case Study – A Novel Therapy for Interstitial Cystitis, Nutrition Education and Consulting Service, May, 2003. Burns RW. 2007. No serious adverse events from 10 years of use. pH Sciences anecdotal data. | |||
| AlkaPlex granules raise pH levels (reduces acidity levels) of body fluids, including urine, blood, and stomach. | Cooper E. 2006. Elite bicyclist study using two levels of Alka-plex® supplementation. Unpublished study, pH Gural M. 2001. The effect of Tummy Tamer™ on urine pH. Unpublished study, pH Sciences. Burns RW, Lund CL. 2003. pH Control™, its effect on urine acidity and implications on blood acidity. Unpublished study, pH Sciences. Konturek JW, Beneke M, Koppermann R, Petersen-Braun M, Weingartner U. The efficacy of hydrotalcite compared with OTC famotidine in the on-demand treatment of gastroesophageal reflux disease: a non-inferiority trial. Med Sci Monit. 2007 Jan;13(1):CR44-9. Thomson AB, Kirdeikis P, Zuk L. Comparison of 200 mg cimetidine with multiple doses of antacid on extent and duration of rise in gastric pH in volunteers. Dig Dis Sci. 1999 Oct;44(10):2051-5. | |||
| AlkaPlex granules help the body maintain a healthy acid-base balance. | Lindinger MI, Franklin TW, Lands LC, Pedersen PK, Welsh DG, Heigenhauser GJ. Role of skeletal muscle in plasma ion and acid-base regulation after NaHCO3 and KHCO3 loading in humans. Am J Physiol. 1999 Jan;276(1 Pt 2):R32-43. Goldfinch J, McNaughton L, Davies P. Induced metabolic alkalosis and its effects on 400-m racing time. Eur J Appl Physiol Occup Physiol. 1988;57(1):45-8. Lobo DN. Fluid, electrolytes and nutrition: physiological and clinical aspects. Proc Nutr Soc. 2004 Aug; 63(3):453-66. Sa pir DG, Chambers NE, Ryan JW. The role of potassium in the control of ammonium excretion during starvation. Metabolism. 1976 Feb; 25(2):211-20. Frassetto L, Morris RC Jr, Sebastian A. Potassium bicarbonate reduces urinary nitrogen excretion in postmenopausal women. J Clin Endocrinol Metab. 1997 Jan;82(1):254-9. Wiederseiner JM, Muser J, Lutz T, Hulter HN, Krapf R. Acute metabolic acidosis: characterization and diagnosis of the disorder and the plasma potassium response. J Am Soc Nephrol. 2004 Jun;15(6):1589. Khanna A, Kurtzman NA.Metabolic alkalosis. Respir Care. 2001 Apr;46(4):354-65.. | |||
| AlkaPlex granules moderate the effects of age-induced metabolic acidosis. | Frassetto L, Sebastian A. Age and systemic acid-base equilibrium: analysis of published data. J Gerontol A Biol Sci Med Sci. 1996 Jan;51(1):B91-9.. Alpern RJ, Sakhaee K. The clinical spectrum of chronic metabolic acidosis: homeostatic mechanisms produce significant morbidity. Am J Kidney Dis. 1997 Feb;29(2):291-302. Frassetto LA. Effect of age on blood acid-base composition in adult humans: role of age-related renal functional decline. Am J Physiol. 1996 Dec;271(6 Pt 2):F1114-22. Frassetto L. Diet, evolution and aging--the pathophysiologic effects of the post-agricultural inversion of the potassium-to-sodium and base-to-chloride ratios in the human diet. Eur J Nutr. 2001 Oct;40(5):200- 13. | |||
| AlkaPlex granules moderate the effects of stress-induced metabolic acidosis | Sahlin K. Metabolic factors in fatigue. Sports Med. 1992 Feb;13(2):99-107. Alpern RJ, Sakhaee K. The clinical spectrum of chronic metabolic acidosis: homeostatic mechanisms produce significant morbidity. Am J Kidney Dis. 1997 Feb;29(2):291-302. Frassetto L. Diet, evolution and aging--the pathophysiologic effects of the post-agricultural inversion of the potassium-to-sodium and base-to-chloride ratios in the human diet. Eur J Nutr. 2001 Oct;40(5):200-13. Maurer MR. Neutralization of Western diet inhibits bone resorption independently of K intake and reduces cortisol secretion in humans. Am J Physiol Renal Physiol. 2003 Jan;284(1):F32-40. Sebastian A. Estimation of the net acid load of the diet of ancestral preagricultural Homo sapiens and their hominid ancestors. Am J Clin Nutr. 2002 Dec;76(6):1308-16. Peters EM, Handjiski B, Kuhlmei A, Hagen E. Neurogenic inflammation in stress-induced termination of murine hair growth is promoted by nerve growth factor. Am J Pathol. 2004 Jul;165(1):259-71. | |||
| AlkaPlex granules aids the body in the removal of acidic waste from cells. | Frassetto L, Morris RC Jr, Sebastian A. Potassium bicarbonate reduces urinary nitrogen excretion in postmenopausal women. J Clin Endocrinol Metab. 1997 Jan;82(1):254-9. Lindinger MI, Franklin TW, Lands LC, Pedersen PK, Welsh DG, Heigenhauser GJ. Role of skeletal muscle in plasma ion and acid-base regulation after NaHCO3 and KHCO3 loading in humans. Am J Physiol. 1999 Jan; 276 (1 Pt 2):R32-43. Goldfinch J, Mc Naughton L, Davies P. Induced metabolic alkalosis and its effects on 400-m racing time. Eur J Appl Physiol Occup Physiol. 1988;57(1):45-8. | |||
| AlkaPlex granules support healthy liver and kidney function. | Alpern RJ, Sakhaee K. The clinical spectrum of chronic metabolic acidosis: homeostatic mechanisms produce significant morbidity. Am J Kidney Dis. 1997 Feb;29(2):291-302. Frassetto L, Morris RC Jr, Sellmeyer DE, Todd K, Sebastian A. Diet, evolution and aging--the pathophysiologic effects of the post-agricultural inversion of the potassium-to-sodium and base-to-chloride ratios in the human diet. Eur J Nutr. 2001 Oct;40(5):200-13. Demigne C, Sabboh H, Remesy C, Meneton P. Protective effects of high dietary potassium: nutritional and metabolic aspects. J Nutr. 2004 Nov;134(11):2903-6. Wiederseiner JM, Muser J, Lutz T, Hulter HN, Krapf R. Acute metabolic acidosis: characterization and diagnosis of the disorder and the plasma potassium response. J Am Soc Nephrol. 2004 Jun;15(6):1589-96. | |||
| Physiological aging of the lungs pushes the acid-base balance in the body toward acid which is moderated by AlkaPlex granules as a dietary supplement. | Brijker F, van den Elshout FJ, Heijdra YF, Bosch FH, Folgering HT. Effect of acute metabolic acid/base shifts on the human airway calibre. Respir Physiol. 2001 Jan;124(2):151-8. Krausz S, Sullivan SF. Cardiorespiratory effects of hypothermia and bicarbonate alkalosis. Pflugers Arch. 1980 Oct; 388(1):79-81. Frassetto L, Morris RC Jr, Sellmeyer DE, Todd K, Sebastian A. Diet, evolution and aging--the pathophysiologic effects of the post-agricultural inversion of the potassium-to-sodium and base-to-chloride ratios in the human diet. Eur J Nutr. 2001 Oct;40(5):200-13. Lin RY, Rehman A. Clinical characteristics of adult asthmatics requiring intubation. J Med. 1995;26(5-6):261-77. | |||
| AlkaPlex granules neutralize the acids generated internally by sustained physical activity (or “exercise-induced metabolic acidosis”). | Hoheisel U, Reinohl J, Unger T, Mense S. Acidic pH and capsaicin activate mechanosensitive group IV muscle receptors in the rat. Pain 110(1-2): 149-57, 2004. Robergs, RA, Ghiasvand F, and Parker D. Lingering construct of lactic acidosis. Am J Physiol Regulatory Integrative Comp Physiol 289(3): R904 - R910, 2005. Boning D, Strobel G, Beneke R, and Maassen N. Lactic acid still remains the real cause of exercise-induced metabolic acidosis. Am J Physiol Regulatory Integrative Comp Physiol 289(3): R902 - R903, 2005. Greenhaff PL, Gleeson M, Maughan RJ. Diet-induced metabolic acidosis and the performance of high intensity exercise in man. Eur J Appl Physiol Occup Physiol. 1988;57(5):583-90. Reidenberg MM, Haag BL, Channick BJ, Shuman CR, Wilson TG. The response of bone to metabolic acidosis in man. Metabolism. 1966 Mar;15(3):236-41. Portington KJ, Pascoe DD, Webster MJ, Anderson LH, Rutland RR, Gladden LB. Effect of induced alkalosis on exhaustive leg press performance. Med Sci Sports Exerc. 1998 Apr;30(4):523-8. Lindinger MI, Franklin TW, Lands LC, Pedersen PK, Welsh DG, Heigenhauser GJ. Role of skeletal muscle in plasma ion and acid-base regulation after NaHCO3 and KHCO3 loading in humans. Am J Physiol. 1999 Jan; 276 (1 Pt 2):R32-43. Ljunghall S, Joborn H, Rastad J, Akerstrom G. Plasma potassium and phosphate concentrations--influence by adrenaline infusion, beta-blockade and physical exercise. Acta Med Scand. 1987;221(1):83-93. Goldfinch J, Mc Naughton L, Davies P. Induced metabolic alkalosis and its effects on 400-m racing time. Eur J Appl Physiol Occup Physiol. 1988;57(1):45-8. Caldwell JE.Diuretic therapy and exercise performance. Sports Med. 1987 Jul-Aug;4(4):290-304. | |||
| AlkaPlex granules promote faster recovery from vigorous workouts. | Robergs R, Hutchinson K, Hendee S, Madden S, Siegler J. Influence of pre-exercise acidosis and alkalosis on the kinetics of acid-base recovery following intense exercise. Int J Sport Nutr Exerc Metab. 2005 Feb;15(1):59-74. Cherry PW, Lakomy HK, Boobis LH, Nevill ME. Rapid recovery of power output in females. Acta Physiol Scand. 1998 Sep;164(1):79. Ratel S, Duche P, Hennegrave A, Van Praagh E, Bedu M. Acid-base balance during repeated cycling sprints in boys and men. J Appl Physiol. 2002 Feb;92(2):479-85. Portington KJ, Pascoe DD, Webster MJ, Anderson LH, Rutland RR, Gladden LB. Effect of induced alkalosis on exhaustive leg press performance. Med Sci Sports Exerc. 1998 Apr;30(4):523-8. Greenhaff PL, Gleeson M, Maughan RJ. Diet-induced metabolic acidosis and the performance of high intensity exercise in man. Eur J Appl Physiol Occup Physiol. 1988;57(5):583-90. Sharp RL, Costill DL, Fink WJ, King DS. Effects of eight weeks of bicycle ergometer sprint training on human muscle buffer capacity. Int J Sports Med. 1986 Feb;7(1):13. Costill DL, Verstappen F, Kuipers H, Janssen E, Fink W. Acid-base balance during repeated bouts of exercise: influence of HCO3. Int J Sports Med, 5(5) 228-231, 1984. Jones NL, Sutton JR, Taylor R, Toews CL. Effect of pH on cardiorespiratory and metabolic responses to exercise. J Appl Physiol, 43 (6) 959-964, 1977. Lindinger MI, Franklin TW, Lands LC, Pedersen PK, Welsh DG, Heigenhauser GJ. Role of skeletal muscle in plasma ion and acid-base regulation after NaHCO3 and KHCO3 loading in humans. Am J Physiol. 1999 Jan; 276 (1 Pt 2):R32-43. Sutton JR, Jones NL, Toews CJ. Effect of PH on muscle glycolysis during exercise. Clin Sci (Lond). 1981 Sep;61(3):331-8. Cooper E. 2006. Elite bicyclist study using two levels of Alka-plex® supplementation. Unpublished study, pH Sciences. | |||
| AlkaPlex granules improves performance during workouts. | Matson LG, Tran ZV. Effects of sodium bicarbonate ingestion on anaerobic performance: a meta analytic review. Int J Sport Nutr. 1993 Mar;3(1):2-28. Harmer AR, McKenna MJ, Sutton JR, Snow RJ. Skeletal muscle metabolic and ionic adaptations during intense exercise following sprint training in humans. J Appl Physiol. 2000 Nov;89(5):1793. Portington KJ, Pascoe DD, Webster MJ, Anderson LH, Rutland RR, Gladden LB. Effect of induced alkalosis on exhaustive leg press performance. Med Sci Sports Exerc. 1998 Apr;30(4):523-8. Caldwell JE. Diuretic therapy and exercise performance. Sports Med. 1987 Jul-Aug;4(4):290-304. Wilkes D, Gledhill N, Smyth R. Effect of acute induced metabolic alkalosis on 800-m racing time. Med Sci Sports Exerc, 15(4) 277-280, 1988. McNaughton LR, Dalton, B, Palmer G. Sodium bicarbonate can be used as an ergogenic aid in high-intensity, competitive cycle ergometry of 1 h duration. Eur J Appl Physiol, 80(1) 64-69, 1999. Webster M.J. 2002. Sodium bicarbonate. In: Bahrke M and Yesalis C, Eds. Performance-enhancing substances in sport and exercise. Champaign, IL: Human Kinetics. p 197-207. Greenhaff PL, Gleeson M, Maughan RJ. Diet-induced metabolic acidosis and the performance of high intensity exercise in man. Eur J Appl Physiol Occup Physiol. 1988;57(5):583-90. Reidenberg MM, Haag BL, Channick BJ, Shuman CR, Wilson TG. The response of bone to metabolic acidosis in man. Metabolism. 1966 Mar;15(3):236-41. Jacobs I, Schele R, Sjodin B. Blood lactate vs. exhaustive exercise to evaluate aerobic fitness. Eur J Appl Physiol Occup Physiol. 1985;54(2):151. McCartney N, Heigenhauser GJ, Jones NL. Effects of pH on maximal power output and fatigue during short-term dynamic exercise. J Appl Physiol. 1983 Jul;55(1 Pt 1):225-9. Busse MW, Maassen N. Effect of consecutive exercise bouts on plasma potassium concentration during exercise and recovery. Med Sci Sports Exerc. 1989 Oct;21(5):489. Cooper E. 2006. Elite bicyclist study using two levels of Alka-plex® supplementation. Unpublished study, pH Sciences. | |||
| AlkaPlex granules decrease the amount of muscle damage and soreness created by vigorous exercise due to the build-up of acids in the muscle. | Haller RG, Lewis SF, Estabrook RW, DiMauro S, Servidei S, Foster DW. Exercise intolerance, lactic acidosis, and abnormal cardiopulmonary regulation in exercise associated with adult skeletal muscle cytochrome c oxidase deficiency. J Clin Invest. 1989 Jul;84(1):155-61. Busse MW, Maassen N. Effect of consecutive exercise bouts on plasma potassium concentration during exercise and recovery. Med Sci Sports Exerc. 1989 Oct;21(5):489. Brien DM, McKenzie DC. The effect of induced alkalosis and acidosis on plasma lactate and work output in elite oarsmen. Eur J Appl Physiol Occup Physiol. 1989;58(8):797-802. Sahlin K. Metabolic factors in fatigue. Sports Med. 1992 Feb;13(2):99-107. Kleger GR, Turgay M, Imoberdorf R, McNurlan MA, Garlick PJ, Ballmer PE. Acute metabolic acidosis decreases muscle protein synthesis but not albumin synthesis in humans. Am J Kidney Dis. 2001 Dec;38(6):1199-207. Vormann J, Worlitschek M, Goedecke T, Silver B. Supplementation with alkaline minerals reduces symptoms in patients with chronic low back pain. J Trace Elem Med Biol. 2001;15(2-3):179-83. Verbitsky O, Mizrahi J, Levin M, Isakov E. Effect of ingested sodium bicarbonate on muscle force, fatigue, and recovery. J Appl Physiol. 1997 Aug;83(2):333-7. | |||
| AlkaPlex granules induce greater muscle alkalinity and supports muscle and athletic endurance (or “time to fatigue”). | Lambert CP, Flynn MG. Fatigue during high-intensity intermittent exercise: application to bodybuilding. Sports Med. 2002;32(8):511-22. Raymer GH, Marsh GD, Kowalchuk JM, Thompson RT. Metabolic effects of induced alkalosis during progressive forearm exercise to fatigue. J Appl Physiol. 2004 Jun;96(6):2050-6. Verbitsky O, Mizrahi J, Levin M, Isakov E. Effect of ingested sodium bicarbonate on muscle force, fatigue, and recovery. J Appl Physiol. 1997 Aug;83(2):333. Sahlin K. Metabolic factors in fatigue. Sports Med. 1992 Feb;13(2):99-107. Cowan RA, Hartnell GG, Lowdell CP, Baird IM, Leak AM. Metabolic acidosis induced by carbonic anhydrase inhibitors and salicylates in patients with normal renal function. Br Med J (Clin Res Ed). 1984 Aug 11; 289 (6441): 347-8. Bushinsky DA. Acid-base imbalance and the skeleton. Eur J Nutr. 2001 Oct;40(5):238-44. Robergs RA, Ghiasvand F, Parker D. Biochemistry of exercise-induced metabolic acidosis. Am J Physiol Regul Integr Comp Physiol. 2004 Sep;287(3):R502-16. Swenson ER. Metabolic acidosis. Respir Care. 2001 Apr;46(4):342-53. Coyle EF. Physiological determinants of endurance exercise performance. J Sci Med Sport. 1999 Oct;2(3):181- 9. Bishop D, Edge J, Davis C, Goodman C. Induced metabolic alkalosis affects muscle metabolism and repeatedsprint ability. Med Sci Sports Exerc. 2004 May;36(5):807-13. Denning H, Talbot JH, Edwards HT, Dill DB. Effect of acidosis and alkalosis upon capacity for work. J Clin Invest, 9, 601-613, 1931. Wijnen S, Verstappen F, Kuipers H. The influence of intravenous NaHCO3 administration in interval exercise: acid-base balance and endurance. Int J Sports Med, 5, 130-132, 1984. Swank A, Robertson RJ. Effect of induced alkalosis on perception of exertion during intermittent exercise. J Appl Physiol, 67(5) 1862-1867, 1989. Burns RW, Lund CL. 2003. pH Control™, its effect on urine acidity and implications on blood acidity. Unpublished study, pH Sciences. | |||
| Exercise-induced metabolic acidosis causes fatigue which is mediated by AlkaPlex based dietary supplements. | Sahlin K. Metabolic factors in fatigue. Sports Med. 1992 Feb;13(2):99-107. Alpern RJ, Sakhaee K. The clinical spectrum of chronic metabolic acidosis: homeostatic mechanisms produce significant morbidity. Am J Kidney Dis. 1997 Feb;29(2):291-302. Frassetto L, Sebastian A. Age and systemic acid-base equilibrium: analysis of published data. J Gerontol A Biol Sci Med Sci. 1996 Jan;51(1):B91-9. Wiederseiner JM, Muser J, Lutz T, Hulter HN, Krapf R. Acute metabolic acidosis: characterization and diagnosis of the disorder and the plasma potassium response. J Am Soc Nephrol. 2004 Jun;15(6):1589. | |||
| AlkaPlex granules alkalize the acids generated internally by high-protein diet (or “diet-induced metabolic acidosis”). | Frassetto LA, Todd KM, Morris RC Jr, Sebastian A. Estimation of net endogenous noncarbonic acid production in humans from diet potassium and protein contents. Am J Clin Nutr. 1998 Sep;68(3):576-83. Marliss EB. Protein diets for obesity: metabolic and clinical aspects. Can Med Assoc J. 1978 Dec 23; 119 (12): 1413-21. Worthington BS, Taylor LE. Balanced low-calorie vs. low-protein-low-carbohydrate reducing diets. II. Biochemical changes. J Am Diet Assoc. 1974 Jan;64(1):52-5. Alpern RJ, Sakhaee K. The clinical spectrum of chronic metabolic acidosis: homeostatic mechanisms produce significant morbidity. Am J Kidney Dis. 1997 Feb; 29 (2):291-302. Frassetto L, Morris RC Jr, Sellmeyer DE, Todd K, Sebastian A. Diet, evolution and aging--the pathophysiologic effects of the post-agricultural inversion of the potassium-to-sodium and base-to-chloride ratios in the human diet. Eur J Nutr. 2001 Oct;40(5):200-13 | |||
| AlkaPlex granules aid the body in the removal of acidic waste from cells. | Frassetto L, Morris RC Jr, Sebastian A. Potassium bicarbonate reduces urinary nitrogen excretion in postmenopausal women. J Clin Endocrinol Metab. 1997 Jan;82(1):254-9. Lindinger MI, Franklin TW, Lands LC, Pedersen PK, Welsh DG, Heigenhauser GJ. Role of skeletal muscle in plasma ion and acid-base regulation after NaHCO3 and KHCO3 loading in humans. Am J Physiol. 1999 Jan;276(1 Pt 2):R32-43. Goldfinch J, McNaughton L, Davies P. Induced metabolic alkalosis and its effects on 400-m racing time. Eur J Appl Physiol Occup Physiol. 1988;57(1):45-8. | |||
| AlkaPlex granules help the body maintain a healthy acid-base balance. | Lindinger MI, Franklin TW, Lands LC, Pedersen PK, Welsh DG, Heigenhauser GJ. Role of skeletal muscle in plasma ion and acid-base regulation after NaHCO3 and KHCO3 loading in humans. Am J Physiol. 1999 Jan;276(1 Pt 2):R32-43. Goldfinch J, Mc Naughton L, Davies P. Induced metabolic alkalosis and its effects on 400-m racing time. Eur J Appl Physiol Occup Physiol. 1988;57(1):45-8. Lobo DN. Fluid, electrolytes and nutrition: physiological and clinical aspects. Proc Nutr Soc. 2004 Aug;63(3):453-66. Sa pir DG, Chambers NE, Ryan JW. The role of potassium in the control of ammonium excretion during starvation. Metabolism. 1976 Feb;25(2):211-20. Frassetto L, Morris RC Jr, Sebastian A. Potassium bicarbonate reduces urinary nitrogen excretion in postmenopausal women. J Clin Endocrinol Metab. 1997 Jan;82(1):254-9. Wiederseiner JM, Muser J, Lutz T, Hulter HN, Krapf R. Acute metabolic acidosis: characterization and diagnosis of the disorder and the plasma potassium response. J Am Soc Nephrol. 2004 Jun;15(6):1589. Khanna A, Kurtzman NA. Metabolic alkalosis. Respir Care. 2001 Apr;46(4):354-65. | |||
| The body is better able to utilize electrolytes in an alkali state induced by AlkaPlex based dietary supplement. | Allison S. Fluid, electrolytes and nutrition. Clin Med. 2004 Nov-Dec;4(6):573-8. Rehrer NJ. Fluid and electrolyte balance in ultra-endurance sport. Sports Med. 2001;31(10):701-15. Demigne C. Protective effects of high dietary potassium: nutritional and metabolic aspects. J Nutr. 2004 Nov; 134 (11):2903-6. Frassetto, L. Diet, evolution and aging--the pathophysiologic effects of the post-agricultural inversion of the potassium-to-sodium and base-to-chloride ratios in the human diet. Eur J Nutr. 2001 Oct;40(5):200-13. Frassetto LA. Estimation of net endogenous noncarbonic acid production in humans from diet potassium and protein contents. Am J Clin Nutr. 1998 Sep;68(3):576-83. | |||
| Certain prescription drugs and trauma push the body’s acid-base balance toward drug induced acidosis which can be mediated by AlkaPlex based dietary supplements. | Neale R, Reynolds TM, Saweirs W. Statin precipitated lactic acidosis? J Clin Pathol. 2004 Sep;57(9):989-90. Jin H, Meyer JM, Jeste DV. Atypical antipsychotics and glucose dysregulation: a systematic review. Schizophr Res. 2004 Dec 1;71(2-3):195-212. Sandhu GK, Heyneman CA. Nephrotoxic potential of selective cyclooxygenase-2 inhibitors. Ann Pharmacother. 2004 Apr;38(4):700-4. Inamasu J, Nakamura Y, Saito R, Kuroshima Y, Mayanagi K, Ohba S, Ichikizaki K. Normokalemia and hyperglycemia in subarachnoid hemorrhage patients resuscitated from prehospital cardiopulmonary arrest. Resuscitation. 2002 Sep; 54(3):255. Hameed SM, Cohn SM. Gastric tonometry: the role of mucosal pH measurement in the management of trauma. Chest. 2003 May;123(5 Suppl):475S. Price G. Metformin lactic acidosis, acute renal failure and rofecoxib. Br J Anaesth. 2003 Dec;91(6):909-10. Boelsterli UA, Zimmerman HJ, Kretz-Rommel A. Idiosyncratic liver toxicity of nonsteroidal antiinflammatory drugs: molecular mechanisms and pathology. Crit Rev Toxicol. 1995; 25(3): 207-35. | |||
| AlkaPlex based dietary supplements reduce acid concentrations in tissue and body fluids with the result that intra-cellular nutrient transportation may be improved. | Abdoun K, Wolf K, Arndt G, Martens H. Effect of ammonia on Na+ transport across isolated rumen epithelium of sheep is diet dependent. Br J Nutr. 2003 Oct;90(4):751-8. Mene P. Transient receptor potential channels in the kidney: calcium signaling, transport and beyond. J Nephrol. 2006 Jan-Feb;19(1):21-9. Wakabayashi I, Poteser M, Groschner K. Intracellular pH as a determinant of vascular smooth muscle function. J Vasc Res. 2006;43(3):238-50. Hayashi H, Szaszi K, Grinstein S. Multiple modes of regulation of Na+/H+ exchangers. Ann N Y Acad Sci. 2002 Nov;976:248-58. Powell JJ, Jugdaohsingh R, Thompson RP. The regulation of mineral absorption in the gastrointestinal tract. Proc Nutr Soc. 1999 Feb;58(1):147-53. Burton RF. The roles of intracellular buffers and bone mineral in the regulation of acid-base balance in mammals. Comp Biochem Physiol Comp Physiol. 1992 Jul;102(3):425-32. | |||
| AlkaPlex granules improve enzyme activity which is very sensitive to tissue acidity conditions. | Eiam-ong S, Laski ME, Kurtzman NA, Sabatini S. Effect of respiratory acidosis and respiratory alkalosis on renal transport enzymes. Am J Physiol. 267(3 Pt 2):F390-9, 1994. Nolan PJ, Knepper MA, Packer RK. Inhibition of IMCD 11 beta-hydroxysteroid dehydrogenase type 2 by low pH and acute acid loading. J Am Soc Nephrol. 8(4):530-4, 1997. Price SR, Wang X, Bailey JL. Tissue-specific responses of branched-chain alpha-ketoacid dehydrogenase activity in metabolic acidosis. J Am Soc Nephrol. 9(10):1892-8, 1998. | |||
| AlkaPlex based dietary supplements reduce the formation of crystals and stones in the urinary tract. | Torres VE, Cowley BD Jr, Branden MG, Yoshida I, Gattone VH. Long-term ammonium chloride or sodium bicarbonate treatment in two models of polycystic kidney disease. Exp Nephrol. 2001;9(3):171-80. Torres VE, Mujwid DK, Wilson DM, Holley KH. Renal cystic disease and ammoniagenesis in Han:SPRD rats. J Am Soc Nephrol. 1994 Nov;5(5):1193-200. Rodman JS. Prophylaxis of uric acid stones with alternate day doses of alkaline potassium salts. J Urol 145(1):97- 9, 1991. Kessler T, Hesse A. Cross-over study of the influence of bicarbonate-rich mineral water on urinary composition in comparison with sodium potassium citrate in healthy male subjects. Br J Nutr 84(6):865-71, 2000. | |||
| AlkaPlex granules release alkalizing minerals slowly so they are available for transport across tissue without overwhelming the transport mechanism. | Johnson EA, Tanford C, Reynolds JA. Variable stoichiometry in active ion transport: theoretical analysis of physiological consequences. Proc Natl Acad Sci U S A. 1985 Aug;82(16):5352-6. Mafe S, Pellicer J, Cervera J. Kinetic modeling of ion conduction in KcsA potassium channel. J Chem Phys. 2005 May 22;122(20):204712. Berteloot A. Kinetic mechanism of Na+ -glucose cotransport through the rabbit intestinal SGLT1 protein. J Membr Biol. 2003 Mar 15;192(2):89-100. | |||
| AlkaPlex granules stay in the system longer for longer-lasting absorption than sodium bicarbonate. | Lindinger MI, Franklin TW, Lands LC, Pedersen PK, Welsh DG, Heigenhauser GJ. Role of skeletal muscle in plasma ion and acid-base regulation after NaHCO3 and KHCO3 loading in humans. Am J Physiol. 1999 Jan; 276 (1 Pt 2):R32-43. Wiederseiner JM, Muser J, Lutz T, Hulter HN, Krapf R. Acute metabolic acidosis: characterization and diagnosis of the disorder and the plasma potassium response. J Am Soc Nephrol. 2004 Jun;15(6):1589-96. Burns, R., Ph.D. Comparing Composition™ with Bicarbonate Alternatives. Unpublished paper, 2004. | |||
| AlkaPlex granules help the body maintain optimal acid-base balance longer than and without the negative side effects of sodium bicarbonate. | Lindinger MI, Franklin TW, Lands LC, Pedersen PK, Welsh DG, Heigenhauser GJ. Role of skeletal muscle in plasma ion and acid-base regulation after NaHCO3 and KHCO3 loading in humans. Am J Physiol. 1999 Jan;276(1 Pt 2):R32-43. Wiederseiner JM, Muser J, Lutz T, Hulter HN, Krapf R. Acute metabolic acidosis: characterization and diagnosis of the disorder and the plasma potassium response. J Am Soc Nephrol. 2004 Jun;15(6):1589-96. Burns, R., Ph.D. Comparing Composition™ with Bicarbonate Alternatives. Unpublished paper, Tamer Laboratories, 2004. | |||
| AlkaPlex granules are significantly more effective than sodium bicarbonate in alkalization. | Lindinger MI, Franklin TW, Lands LC, Pedersen PK, Welsh DG, Heigenhauser GJ. Role of skeletal muscle in plasma ion and acid-base regulation after NaHCO3 and KHCO3 loading in humans. Am J Physiol. 1999 Jan;276(1 Pt 2):R32-43. Wiederseiner JM, Muser J, Lutz T, Hulter HN, Krapf R. Acute metabolic acidosis: characterization and diagnosis of the disorder and the plasma potassium response. J Am Soc Nephrol. 2004 Jun;15(6):1589-96. Burns, R., Ph.D. Comparing Composition™ with Bicarbonate Alternatives. Unpublished paper, 2004. | |||
| The absorbed alkaline materials of AlkaPlex mediate the acid-producing phase of the localized inflammatory response to injury. |
|
|||
| The absorbed alkaline materials of AlkaPlex granules can moderate the cycle of chronic inflammation induced by over acidity of tissue. | Losso JN, Bawadi HA. Hypoxia inducible factor pathways as targets for functional foods. J Agric Food Chem 53 (10): 3751-68, 2005. formate intoxication- role of the Fenton reaction. Proc Natl Acad Sci U S A 98(24): 13549-13553, 2001. Komarova SV, Pereverzev A, Shum JW, Sims SM, Dixon SJ. Convergent signaling by acidosis and receptor activator of NF-kappaB ligand (RANKL) on the calcium/calcineurin/NFAT pathway in osteoclasts. Proc Natl Acad Sci U S A 102(7):2643-8, 2005. Serrano CV Jr, Fraticelli A, Panniccia R, Teti A, Noble B. pH dependence of neutrophil-endothelial cell adhesion and adhesion molecule expression. Am J Physiol 271(3 Pt 1):C962-70, 1996. Yamaura K, Akiyoshi K, Irita K, Taniyama T, Takahashi S. Effects of olprinone, a new phosphodiesterase inhibitor, on gastric intramucosal acidosis and systemic inflammatory responses following hypothermic cardiopulmonary bypass. Acta Anaesthesiol Scand 45(4):427. Zambon JJ, Mather ML, Gonzales Y. A microbiological and clinical study of the safety and efficacy of baking-soda dentifrices. Compend Contin Educ Dent Suppl 18(21):S39-44, 1997. Keay SK, Szekely Z, Conrads TP, Veenstra TD, Barchi JJ Jr. An antiproliferative factor from interstitial cystitis patients is a frizzled 8 protein-related sialoglycopeptide. Proc Natl Acad Sci U S A 101(32):11803-8, 2004. Parsons CL. Successful downregulation of bladder sensory nerves with combination of heparin and alkalinized lidocaine in patients with interstitial cystitis. Urology 65(1):45-8, 2005. Dell JR, Parsons CL. Multimodal therapy for interstitial cystitis. J Reprod Med 49(3 Suppl):243-52, 2004. Gillespie L. Metabolic appraisal of the effects of dietary modification on hypersensitive bladder symptoms. Br J Urol. 1993 Sep;72(3):293-7. Nickel JC. Interstitial cystitis. Etiology, diagnosis, and treatment. Can Fam Physician. 2000 Dec;46(12):2430-4, 2437-40. Chung MK. Interstitial cystitis in persistent posthysterectomy chronic pelvic pain. JSLS. 2004 Oct- Dec;8(4):329-33 . Dallosso HM, McGrother CW, Matthews RJ, Donaldson MM. The association of diet and other lifestyle factors with overactive bladder and stress incontinence: a longitudinal study in women. BJU Int 92(1):69-77, 2003. | |||
| AlkaPlex granules attenuate the activation of sensory neurons associated with the acid-producing phase of the inflammatory response. | Steen KH, Steen AE, Reeh PW. A dominant role of acid pH in inflammatory excitation and sensitization of nociceptors in rat skin, in vitro. J Neurosci 15(5 pt 2):3982-9, 1995. Yiangou Y, Facer P, Smith JA, Sangameswaran L, Eglen R. Increased acid-sensing ion channel ASIC-3 in inflamed human intestine. Eur J Gastroenterol Hepatol 13(8):885-8, 2001. Mamet J, Baron A, Lazdunski M, Voilley N. ProInflammatory mediators, stimulators of sensory neuron excitablity via the expression of acid-sensing ion channels. J Neuroscience 22(24): 10662-70, 2002. Davies RJ. Buffering the pain of local anaesthetics: A systematic review. Emerg Med (Fremantle) 15(1):81-8, 2003. Vossinakis IC, Stavroulaki P, Paleochorlidis I, Badras LS. Reducing the pain associated with local anaesthetic infiltration for open carpal tunnel decompression. J Hand Surg [Br] 29(4):399-401, 2004. Vormann J, Worlitschek M, Goedecke T, Silver B. Supplementation with alkaline minerals reduces symptoms in patients with chronic low back pain. J Trace Elem Med Biol 15(2-3):179-83, 2001. |